Do I have COVID-19? Reviewing my Pediatric COVID-19 Lectures Notes. I’d Rather Remind You About VACCINES.

August 7, 2020
by drplasticpicker
I may or may not have been exposed to COVID-19. I may or may not have COVID-19. I’m in the same boat as many through the world. I’ve been wearing double mask, faceshield, and washing hands at every patient encounter. We haven’t really gone much of anywhere other than work and grocery store. I have been careful.
But life happens and the COVID-19 pandemic is slowly making it’s way through our population. I’m isolated in our bedroom waiting with only the puppy visiting, and waiting for my Health Care Worker expediated test results which should be tonight. I’m taking this opportunity to review the recent Pediatric COVID-19 lectures. It doesn’t really help to worry, so I’ll just study.
In our area right now it’s about 12% COVID-19 PCR positivity rate, and COVID-19 serologiess are at 11% positive. We had peaked at 19% COVID-19 PCR positivity rate, and right now it is trending down. But infectious disease states we should expect ebbs and flows. Hospitalizations are down in our particular area. I actually don’t think I have COVID-19. I don’t think it would be this easy, but I do not want to put my patients at risk and will wait to see what the test results are.
Take Home Points for Me This Week Regarding COVID-19.
- Cycle Threshold Values (CT) indicates amount of viral nucleic acid in the upper respiratory tract system. When I heard this in the ID lecture, I was confused. But all a Cycle Threshold (CT) Value is “The Ct value is associated with the amount of PCR product in the reaction. The lower the Ct value, the more PCR product that is present. This is because it takes fewer PCR cycles for that product to be detected over the background signal.” https://toptipbio.com/ct-value-qpcr/ Therefore in recent studies younger children were found to have significantly lower CT values than older children/adults, which means they have more viral nucleic acid in their upper respiratory system. The observed difference indicates a 10-100X difference in the amount of SARS-CoV-2. This does not surprise any pediatrician. We all know young kids are germbags! Ask any third year medical student doing their pediatrics rotation, they think those toddlers are cute until they get sick with diarrhea during their rotations! LOL.
- We Don’t Know If This Means Young Children Are More Contagious! I texted a colleague about COVID-19, and I ended our exchange with “All I know about COVID-19 is no one knows nothing.” Honestly that is how I feel sometimes as a front-line pediatrician. We don’t know if increased viral nucleic acid particles are actually infectious. The funniest part of the lecture was when the infectious disease specialist made the astute observation that little kids may not be an infectious because “the height of the child, you know, if it’s going fall to the knees and drop.” Essentailly that since they are closer to the ground, than any secretions will fall to the ground quicker. That is a valid but still hilariously funny comment.
- You can Get It at Camp! I’m not sure why people are surprised of this. I’ve heard of folks sending their kids to camp. I am not their pediatrician and did not comment. But in one Georgia Sleep Away camp, the “attack rate” of COVID-19 positivity when one camper had it was 44%. Yep. You’ll get it at camp especially sleep away camp.
- Not A Lot Of Kids are Dying of COVID-19: I was trying to reassure our tween daughter. She worries more than others and since I’m quarantined in my bedroom right now, she is worried. Mainstream media and disinformation are not helping. Yes we would all shelter in place as much as possible, wear a mask, wash hands, stay six-feet away from everyone – but let us not forget facts. We are 5 months into this pandemic, and ONE CALIFORNIA CHILD HAS DIED FROM COVID-19. Yes there are other consequences of COVID-19, but in terms of actual death – One child. For children under 14 years of age, in the ENTIRE USA of the 135, 579 deaths due for COVID-19 there have been 42 children. That is 0.00031 % of the deaths have been due to children under 14 years of age.
- Most People with COVID-19 are doing fine and even after Diagnosing Do Not Need to Be Monitored. So far only 6% of patients who are diagnosed with COVID-19 in the ED/Outpatient are later readmitted, and that group’s overall mortality rate is 0.6%. If you are younger than 65 years of age, the mortality is 0.3%. I have been calling people trying to reassure them and sometimes doing close phone follow up. It makes the parents feel better, but honestly I could probably stop. Mostly I’m offering it for their mental health.
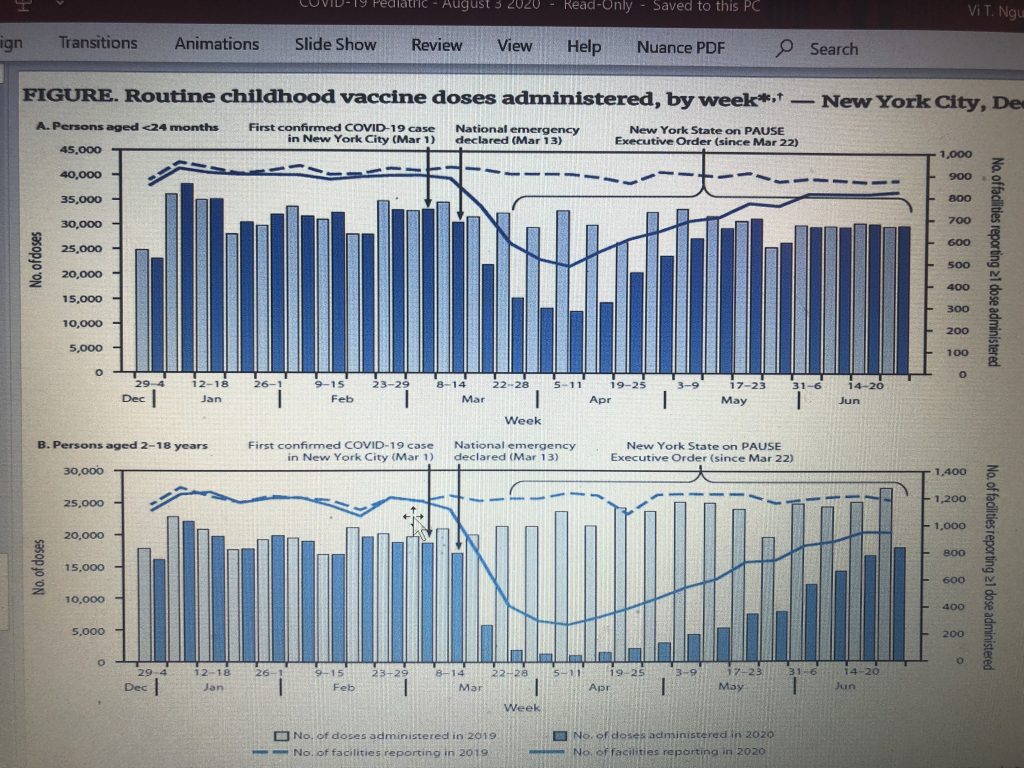
- 6. Dropping Vaccine Rates During Quarantine Pose a Greater Risk to Children than COVID-19: Review the graph below. Everyone in clinic persists on asking me about COVID-19 minutiae like when this hypothetical vaccine is going to happen and whether it is being rushed. I honestly looked at the parents in my practice and said that I am not a vaccine expert, nor an infectious disease doctor, and it does not effect my practice and ability to care for my patients right now. I am a front-line pediatrician, and when that data starts coming than I’ll review it as part of our collective group. Right now, I’m focused on the vaccines we already have and getting kids vaccinated in a safe environmentally, while masked and good handwashing. What is more likely to hurt your child is strep pneumonia, a common bacterial pathogen in our own respiratory system. This is given at the 2 mo, 4 mo, 6 mo, 12 mo and 4 year old visits. “
Pneumococcal disease can be very serious.
- Pneumococcal pneumonia causes an estimated 150,000 hospitalizations each year in the United States.
- Pneumococcal meningitis and bacteremia killed approximately 3,600 people in the United States in 2017. https://www.cdc.gov/pneumococcal/about/facts.html
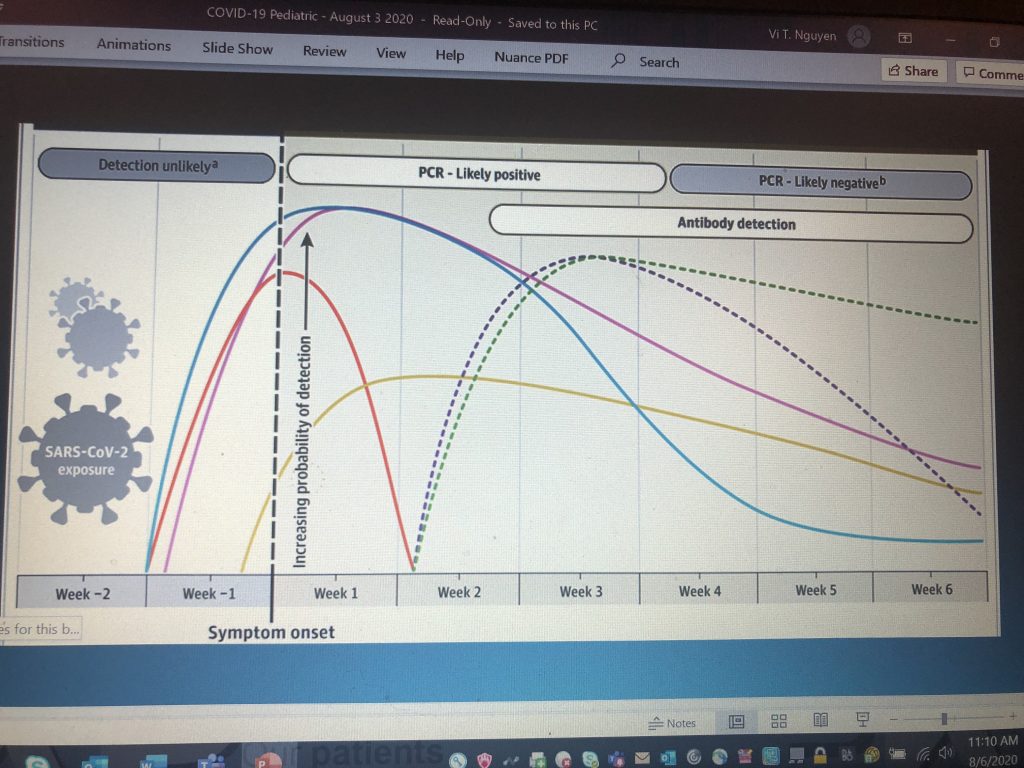
7. COVID-19 Testing Has It’s Limitations and Needs to Be Timed Appropriately. I love how everyone expects doctors to be essentially like Phlox in Star Trek Enterprise with a medical tricorder. As if I can just take my HMO iphone and scan your body with a remote device up and down, and tell you what you have! The technology is not there yet, and I don’t think medicine ever will work that way. Medical test have false negatives, false positives, positive predictive values, negative predictive values, sensitivity and specificity. Epidemiology is one of the classes I made sure to pay close attention to my second year, and even then it was much more complicated than you can imagine. I am as good as any front-line physician at interpreting these values and have a few published research articles (I don’t think anyone read?) – but even I need to open up a statistics website to review what those things mean. In general, testing is not perfect and it is complicated and depends on many many factors including how well someone did the test, what the current disease prevalence is in the community, and the specific test used. Test results are not TRUTH. For asymptomatic high risk exposures (unmasked more than 15 minutes within 6-feet of a confirmed COVID-19 person), than it’s best to test 5-7 days after exposure. And even then, that person can still develop symptoms after a negative test because the incubation period is 14 days. They still need to take standard precautions for tasking and social distancing and quarantine for 14 days from last exposure date. It only makes sense to test folks right now because of still national limited test capacity if it will change their behavior and those who will put significant people at risk like Health Care Workers. Everyone else should quarantine anyway. We should treat everyone right now like they have COVID-19. If you are ill, it’s best to check within the first week when one actually has symptoms. For me that is fever, cough, sore throat, headache, body aches and loss of smell. So far, these are the symptoms that have been tried in true for the COVID-19 patients that I have treated. Today, while waiting for my results – I have none of those symptoms really. Antibody teseting is most helpful again after idividuals have completed their illness after 10-14 days. I have not tested anyone for antibodies because we don’t yet know if having antibodies will give people protection for a second onslaught of COVID-19, and it has not changed treatment and recommendations.
These are just my thoughts after reviewing my lecture notes, as I use this blog as a way to study. It makes me reassured that after my exposure that COVID-19 is still a relatively mild and survivable disease for a majority of the population especially children 14 and under. I did get to go through the COVID-19 test, which was horrible! OMG I never want to go through that again. I’m sure the disease itself is even more horrible. The reason we are all taking serious measures to contain COVID-19 is that because very few of us have had it. Even though the death rate is low – hundreds of thousands will die by December because even 0.6% death rate multiplied by millions of people equates to hundreds of thousands of deaths of mostly our beloved grandparents.
In conclusion, please still follow public health orders. Wear your mask. Wash hands. Stay mostly six feet apart. Reassure your children they are doing this because we are making sure adults/grandparents stay healthy until we get a vaccine. We want to ensure we have enough room in the hospitals to slowly take care of this slow burn. But in the whole state of California only ONE CHILD HAS DIED OF COVID-19, whereas in the country every year 3,600 people die of pneumococcal disease. This includes many young children after the age of 2. So please bring your kids in for their vaccines. All of them.
*Disclaimer: This blog is for entertainment purposes and information is delivered in a hopefully funny and approachable way, but I AM NOT DOCTOR OF THE ENTIRE INTERNET. For actual personal medical advice, go to your own doctor and ask your own pediatrician. If you want actual advice about COVID-19, go to the CDC or your local health agency. If I’m your pediatrician, than I’ll “see” you in the office and contact me through the normal patient portal. This is my study notes while I am reviewing lecture notes and I may have COVID-19, and maybe encephalopathic! It’s always possible. That’s my story and I’m sticking to it! Plus next weeks’ covid-19 information will probably be totally different. Things are changing super fast.
